Our forYOU team has been recognized nationally as a leader in supporting our caregivers. We are often contacted by health care providers outside MU Health Care who would like to learn more about our research or use our materials as a model for developing similar programs. Please feel free to use the information and materials on these pages, including our brochures. For more information, please email us or call us at 573-884-2373.
Caring for Caregivers
Most health care providers adjust well to the multitude of demands encountered during an unexpected or traumatic clinical event. Providers often have strong emotional defenses that carry them through and let them "get the job done." Yet sometimes the emotional aftershock (or stress reaction) can be difficult. Signs and symptoms of this emotional aftershock may last a few days, a few weeks, a few months, or longer.
Second victims are "health care providers who are involved in an unanticipated adverse patient event, medical error and/or a patient related injury and become victimized in the sense that the provider is traumatized by the event."
Frequently, second victims:
- Feel personally responsible for the unexpected patient outcomes
- Feel as though they have failed the patient
- Second-guess their clinical skills
- Second-guess their knowledge base
Second Victim Fast Facts
- Each second victim (even those involved in the same event) will have unique experiences and needs
- Regardless of job title, providers respond in predictable manners. The six stages of second victim recovery explain how the second victim is impacted by the clinical event
- There are some events that are high risk for inducing a second victim response
- First tendency of providers is self isolation
- Providers tend to 'worry' in a predictable pattern
- Sometimes the entire team is impacted by a clinical event
High-risk Scenarios and Recovery Stages
There are several types of clinical events that can evoke a second victim response. Examples of high-risk situations that may induce a stress response include:
- Patient who “connects” to a health care professional’s own family
- Unanticipated clinical event involving a pediatric patient
- Unexpected patient death
- Preventable harm to patient
- Multiple patients with bad outcomes within a short period of time within one clinical area
- Long-term care relationship with patient death
- Clinician experiencing his or her first patient death
- Failure to detect patient deterioration in timely manner
- Death in a young adult patient
- Notification of pending litigation plans
- Community high-profile patient or event
- Health care professional who experienced needle stick exposure with high-risk patient
- Death of a staff member or spouse of a staff member
Recovery Stages
Healing and recovery occurs in a predictable manner.
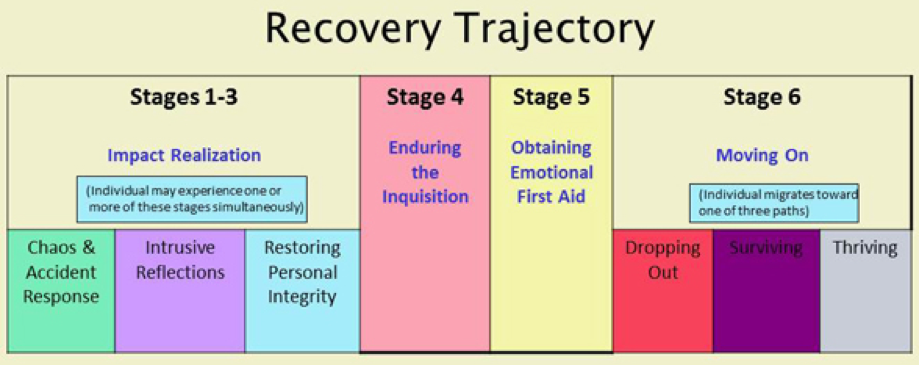
Six stages of second victim recovery have been identified as:
- Chaos and Accident Response
- Intrusive Reflections
- Restoring Personal Integrity
- Enduring the Inquisition
- Obtaining Emotional First Aid
- Moving On
- Dropping out
- Surviving
- Thriving
Download a handout with more details about the second victim recovery trajectory (PDF).
Triggering has been defined as reliving the initial event when an external stimulus, such as a similar clinical situation, is presented. Triggering may occur at any time following the event by a random number of variables that the caregiver encounters.
Different factors have been described as triggering fresh memories of an old event. Examples of common triggers are taking care of a patient in the exact location of the original event, treating a patient with a similar name or similar diagnosis or treating of the original patient. When the memory is triggered, similar physical or psychological symptoms may return.
Common Responses and Symptoms
Distressed caregivers follow predictable patterns of worrying about:
| Patient | Me | Peers | |
|---|---|---|---|
| Is the patient/family okay? | Will I be fired? | What will my colleagues think? | |
| What have they been told? | Will I be sued? | Will I ever be trusted again | |
| How did they respond? | Will I lose my license? | Will I still be a respected member of my team? |
Next Steps
- Who will contact me to discuss the case?
- If a lawsuit does happen, when will I know? How will I hear about it?
- What do I need to do?
Common Phrases
- “I had a sickening realization of what happened.”
- “I don't deserve to be a doctor.”
- “This will change the way I come to work from now on.”
- “This has been a career-changing event.”
- “I came to work today to help someone, not to hurt them.”
- “This is a turning point in my career.”
- “This event shook me to my core. I’ll never be the same again.”
Signs and Symptoms
Second victims experience various physical and psychosocial symptoms. These symptoms are normal reactions to an abnormal and unanticipated patient event or outcome.
Common reactions reported by distressed caregivers include several psychological and physical symptoms.
| Physical Symptoms | Psychological Symptoms |
|---|---|
| Sleep disturbances | Isolation |
| Difficulty concentrating | Frustration |
| Eating disturbances | Fear |
| Headache | Uncomfortable returning to work |
| Fatigue | Anger, Irritability |
| Nausea, vomiting | Depression |
| Diarrhea | Extreme Sadness |
| Rapid heart rate | Self-doubt |
| Rapid breathing | Flashbacks |
| Muscle tension | Feeling numb |
Downloadable Materials (PDFs)
- forYOU Brochure for Employees
- forYOU Brochure for Family Members
- Six Stages of Recovery Handout
- The Scott Three-Tiered Interventional Model of Second Victim Support
Publications
- Burlison, J.D., Quillivan, R.R., Scott, S.D., Johnson, S. and Hoffman, J.M. (2016). The effects of the second victim phenomenon on work-related outcomes: Connecting caregiver distress to turnover intentions and absenteeism.Patient Safety & Quality Healthcare. November 2, 2016.doi: 10.1097/PTS.0000000000000301.
- Quillivan, R.R., Burlison, J.D., Browne, E.K., Scott, S.D., and Hoffman, J.M. (2016). Patient safety culture and the second victim phenomenon: Connecting culture to staff distress in nurses. The Joint Commission Journal on Quality and Patient Safety.42(8)377-386(10).
- Scott, S.D. & McCoig, M. (2016). Care at the point of impact – Insights into the second victim experience. Journal of Healthcare Risk Management. 35(4),6-13.
- VanGerven, E., Deweer, D., Scott, S.D., Panella, Massimiliano, P., Euwena, M., Serneus, W. & Vanhaecht. (2016, April) Personal, situational, and organizational determinants of the impact on physicians, nurses and midwives as second victims after a patient safety incident: A qualitative study. Journal of the Spanish Society for Quality Assurance. doi:10.1016/j.cali.2016.02.003.
- Scott, S.D. (2015). Second victim support: Implications for patient safety attitudes and perceptions. Patient Safety & Quality Healthcare. 12(5), 26-31.
- Miller, R.G., Scott, S.D., and Hirschinger, L.E. (2015). Improving patient safety: The intersection of safety culture, clinician and staff support, and patient safety organizations. Center for Patient Safety; Jefferson City, Missouri. September 2015.
- Scott, S.D. (2015). The second victim experience: Mitigating the harm. American Nurse Today. September 2015. 10(9),8-11.
- Hirschinger, L.E., Scott, S.D, and Hahn-Cover, K. (2015). Clinician support: Five years of lessons learned. Patient Safety & Quality Healthcare.12(2),26-31.
- Burlison, J., Scott, S.D., Browne, E., Thompson, S., & Hoffman, J.M. (2014). The second victim experience and support survey: measuring healthcare providers’ responses to unanticipated adverse patient safety events and levels of support. The Joint Commission Journal on Quality and Patient Safety. [Published online ahead of print August 26 2014]. doi: 10.1097/PTS.0000000000000129.
- Scott, S.D. & Hahn-Cover, K. (2013). The second victim phenomenon. In Patient Safety: A Case-Based Comprehensive Guide. Springer Publishing. October 2013.
- Seys, D.,Wu, A.W., VanGerven, Vleugels, A., Euwema, M., W., Panella, M., Scott, S.D., Conway, J, Sermeus, W., and Vanhaecht. (2012). Second victims after adverse events: a literature review. Evaluation and the Health Professions. September, 1-28.
- Seys, D., Scott, S.D., Wu, A.W., VanGerven, E., Vieugels, A., Euwema, M., Panella, M. Conway, J., and Vanhaecht, K. (2012). Supporting involved health care professionals (second victims) following an adverse health event: a literature review. International Journal of Nursing Studies. July 30, 2012
- Hall, L.W. and Scott, S.D. (2012). The second victim of adverse health care events. Nursing Clinics of North America.47(3):383-393.
- Pratt, S., Kenney, L., Scott, S.D., and Wu, A.W. (2012) How to develop a second victim support program: a toolkit for healthcare organizations. Quality and Safety in Health Care, 38(5):235-240
- Babak, S. and Scott, S.D. (2010). Rapid response systems: From implementation to evidence-base. The Joint Commission Journal on Quality and Patient Safety, 36(11):514-517.
- Scott, S.D. The second victim phenomenon: A harsh reality of health care professions[Perspective]. AHRQ WebM&M [serial online]. May 2011.
- Scott, S.D., Hirschinger, L.E., McCoig, M.M., Cox, K.R., Hahn-Cover, K., & Hall, L.W. (2011) The second victim. In M.A. DeVita, K. Hillman, & R. Bellomo (Eds.). Textbook of rapid response systems (pp. 321-330). New York, NY: Springer.
- Brandt, J., Cox, K.R., Hall, L.W., Hirschinger, L.E. McCoig, M.M. and Scott, S.D. (2010). Second victims: Mitigating the impact on health care team members following an adverse clinical event. American Journal of Medical Quality Supplement, 25 (2):27S.
- Scott, S.D., Hirschinger, L.E., Cox, K.R., McCoig, M.M., Hahn-Cover, K., Epperly, K.M., Hall, L.W. (2010). Caring for our own: Developing a systemwide second victim rapid response team. Journal on Quality and Patient Safety, 36(5), 233-240.
- Cox, K.R., Scott, S.D., Hall, L.W., Aud, M.A., Headrick, L.A., and Madsen, R. (2009). Uncovering Differences Among Health Professions Trainees Exposed to an Interprofessional Patient Safety Curriculum. Quality Management in Health Care. July-September, 18(3),182-193.
- Hall, L.W., Hahn-Cover, K., Scott, S.D. (2010). The human side of medical errors. The Virtual Lecture Hall, Medical Directions, Inc.; Computerized CME Learning Module.
- Scott, S.D., Hirschinger, L.E., Cox, K.R., McCoig, M.M., Brandt, J., & Hall, L.W. (2009). The natural history of recovery for the health care provider 'second victim' after adverse patient events. Quality Safety in Health Care, 18, 325-330.
- Scott, S.D., Hirschinger, L.E. & Cox, K.R. (2008) Sharing the load: Rescuing the healer after trauma. RN, 71. 38-43.